You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
High cholesterol
- Thread starter vincsho
- Start date
More options
Who Replied?This is absolute lies.The best medicine is no need medications, just be vegetarian or vegan and it will come down naturally. Remember your alimentary canal is designed for vegetarian food..
Humans are obligate carnivores.
Our gut cannot ferment and break down cellulose like herbivores and is highly acidic like carnivores.
Nature don't lies, it's humans self deceived. You have the absolute free will to choose your path and pay the price.This is absolute lies.
Humans are obligate carnivores.
Our gut cannot ferment and break down cellulose like herbivores and is highly acidic like carnivores.
It is always amusing seeing zealots from various food camps duking out with their own hypothesis.
Suffice to say
1) TG is an independent risk indicator for ASCVS
2) LDL is also an independent risk factor, also shown to be causative. Reduction of High LDL via lifestyle or drugs showed direct reduction in CVS mortality.
3) Apo B is a better marker of CVS risk than LDL or TG, and LDL generally correlates with Apo B, though there are cases of discordances. 90% of all Apo B is found in LDL, with the 10% in VLDL and IDL.
4) As for CVS risk of different LDL particle size, small dense LDL penetrate the endothelium more readily, but large fluffy LDL carry more atherogenic ingredient. Thus no net difference and all LDL are considered atherogenic.
5) There is no hard evidence to suggest LMHR with high LDL has a lower CVS risk than normal cohort with high LDL or high LDL is considered safe, despite all the noise in social media. It will be interesting to follow actual prevalence of CVS cases in this cohort. While waiting for this puzzle to reveal, it is important to note that there are cases of LMHR having CVS events in the literature such as below.
https://www.ahajournals.org/doi/10.1161/circ.148.suppl_1.17807
Introduction: Ketogenic diet (KD) has been a popular diet method for weight loss and described as an alternative to pharmacotherapy on social media. KD is thought to improve some risk factors of ASCVD, such as type 2 DM, obesity, and decrease LDL. Recent studies have described lean mass hyper-responders (LMHR), a specific phenotype with lower BMI, total cholesterol >200 mg/dL, HDL >80, and TG <70. LMHR is thought to be protective against ASCVD. While on carbohydrate restricted diet, LMHR may have significant rise in LDL. We present a patient with known CAD and similar phenotype to LMHR that developed rapid progression of CAD after stopping statin and initiating strict KD.
Hypothesis: KD may accelerate disease in those with known CAD, despite being LMHR phenotype.
Methods: 51-year-old male with BMI 23, CAD with previous PCI to proximal LAD, HTN, HLD, family history of early CAD, presented with inferior STEMI. He underwent emergent catheterization revealing 95% stenosis of the mid RCA and 99% occlusion of the distal RCA treated with two drug eluting stents. Previous catheterization showed only moderate disease of the distal RCA. He had discontinued atorvastatin about 2 years after his first coronary intervention due to myalgias. Prior to starting it, his total cholesterol was 207, LDL 131, HDL 43, and TG 67 with a normal BMI- similar traits to LMHR phenotype. Atorvastatin 80 mg was started, and his LDL decreased to 44. After he discontinued the statin, he started a KD to try to manage his cholesterol and CAD.
Results: When he presented with STEMI, his total cholesterol was 388, LDL 301, HDL 73, TG 71, and Lp(a) 155 nmol/L. He resumed atorvastatin 80 mg and started alirocumab at discharge with subsequent LDL of 14.
Conclusions: Social media has influenced many to try ketogenic diet to manage metabolic health. Some influencers have questioned high-LDL association with ASCVD and have recommended avoiding pharmacotherapy. Despite popular opinion that high-LDL in this phenotype does not have clinical implication, our patient with a similar profile had rapid progression of CAD while on a KD and was untreated for HLD. Patients with known CAD and LMHR should be very cautious when starting popular diets and should discuss the possible implications with their provider.
Suffice to say
1) TG is an independent risk indicator for ASCVS
2) LDL is also an independent risk factor, also shown to be causative. Reduction of High LDL via lifestyle or drugs showed direct reduction in CVS mortality.
3) Apo B is a better marker of CVS risk than LDL or TG, and LDL generally correlates with Apo B, though there are cases of discordances. 90% of all Apo B is found in LDL, with the 10% in VLDL and IDL.
4) As for CVS risk of different LDL particle size, small dense LDL penetrate the endothelium more readily, but large fluffy LDL carry more atherogenic ingredient. Thus no net difference and all LDL are considered atherogenic.
5) There is no hard evidence to suggest LMHR with high LDL has a lower CVS risk than normal cohort with high LDL or high LDL is considered safe, despite all the noise in social media. It will be interesting to follow actual prevalence of CVS cases in this cohort. While waiting for this puzzle to reveal, it is important to note that there are cases of LMHR having CVS events in the literature such as below.
https://www.ahajournals.org/doi/10.1161/circ.148.suppl_1.17807
Introduction: Ketogenic diet (KD) has been a popular diet method for weight loss and described as an alternative to pharmacotherapy on social media. KD is thought to improve some risk factors of ASCVD, such as type 2 DM, obesity, and decrease LDL. Recent studies have described lean mass hyper-responders (LMHR), a specific phenotype with lower BMI, total cholesterol >200 mg/dL, HDL >80, and TG <70. LMHR is thought to be protective against ASCVD. While on carbohydrate restricted diet, LMHR may have significant rise in LDL. We present a patient with known CAD and similar phenotype to LMHR that developed rapid progression of CAD after stopping statin and initiating strict KD.
Hypothesis: KD may accelerate disease in those with known CAD, despite being LMHR phenotype.
Methods: 51-year-old male with BMI 23, CAD with previous PCI to proximal LAD, HTN, HLD, family history of early CAD, presented with inferior STEMI. He underwent emergent catheterization revealing 95% stenosis of the mid RCA and 99% occlusion of the distal RCA treated with two drug eluting stents. Previous catheterization showed only moderate disease of the distal RCA. He had discontinued atorvastatin about 2 years after his first coronary intervention due to myalgias. Prior to starting it, his total cholesterol was 207, LDL 131, HDL 43, and TG 67 with a normal BMI- similar traits to LMHR phenotype. Atorvastatin 80 mg was started, and his LDL decreased to 44. After he discontinued the statin, he started a KD to try to manage his cholesterol and CAD.
Results: When he presented with STEMI, his total cholesterol was 388, LDL 301, HDL 73, TG 71, and Lp(a) 155 nmol/L. He resumed atorvastatin 80 mg and started alirocumab at discharge with subsequent LDL of 14.
Conclusions: Social media has influenced many to try ketogenic diet to manage metabolic health. Some influencers have questioned high-LDL association with ASCVD and have recommended avoiding pharmacotherapy. Despite popular opinion that high-LDL in this phenotype does not have clinical implication, our patient with a similar profile had rapid progression of CAD while on a KD and was untreated for HLD. Patients with known CAD and LMHR should be very cautious when starting popular diets and should discuss the possible implications with their provider.
Last edited:
Interesting case studies.It is always amusing seeing zealots from various food camps duking out with their own hypothesis.
Suffice to say
1) TG is an independent risk indicator for ASCVS
2) LDL is also an independent risk factor, also shown to be causative. Reduction of High LDL via lifestyle or drugs showed direct reduction in CVS mortality.
3) Apo B is a better marker of CVS risk than LDL or TG, and LDL can be considered as a subset of Apo B. 90% of all Apo B is found in LDL, with the 10% in VLDL and IDL.
4) As for CVS risk of different LDL particle size, small dense LDL penetrate the endothelium more readily, but large fluffy LDL carry more atherogenic ingredient. Thus no net difference and all LDL are considered atherogenic.
5) There is no hard evidence to suggest LMHR with high LDL has a lower CVS risk than normal cohort with high LDL or high LDL is considered safe, despite all the noise in social media. It will be interesting to follow actual prevalence of CVS cases in this cohort. While waiting for this puzzle to reveal, it is important to note that there are cases of LMHR having CVS events in the literature such as below.
https://www.ahajournals.org/doi/10.1161/circ.148.suppl_1.17807
Introduction: Ketogenic diet (KD) has been a popular diet method for weight loss and described as an alternative to pharmacotherapy on social media. KD is thought to improve some risk factors of ASCVD, such as type 2 DM, obesity, and decrease LDL. Recent studies have described lean mass hyper-responders (LMHR), a specific phenotype with lower BMI, total cholesterol >200 mg/dL, HDL >80, and TG <70. LMHR is thought to be protective against ASCVD. While on carbohydrate restricted diet, LMHR may have significant rise in LDL. We present a patient with known CAD and similar phenotype to LMHR that developed rapid progression of CAD after stopping statin and initiating strict KD.
Hypothesis: KD may accelerate disease in those with known CAD, despite being LMHR phenotype.
Methods: 51-year-old male with BMI 23, CAD with previous PCI to proximal LAD, HTN, HLD, family history of early CAD, presented with inferior STEMI. He underwent emergent catheterization revealing 95% stenosis of the mid RCA and 99% occlusion of the distal RCA treated with two drug eluting stents. Previous catheterization showed only moderate disease of the distal RCA. He had discontinued atorvastatin about 2 years after his first coronary intervention due to myalgias. Prior to starting it, his total cholesterol was 207, LDL 131, HDL 43, and TG 67 with a normal BMI- similar traits to LMHR phenotype. Atorvastatin 80 mg was started, and his LDL decreased to 44. After he discontinued the statin, he started a KD to try to manage his cholesterol and CAD.
Results: When he presented with STEMI, his total cholesterol was 388, LDL 301, HDL 73, TG 71, and Lp(a) 155 nmol/L. He resumed atorvastatin 80 mg and started alirocumab at discharge with subsequent LDL of 14.
Conclusions: Social media has influenced many to try ketogenic diet to manage metabolic health. Some influencers have questioned high-LDL association with ASCVD and have recommended avoiding pharmacotherapy. Despite popular opinion that high-LDL in this phenotype does not have clinical implication, our patient with a similar profile had rapid progression of CAD while on a KD and was untreated for HLD. Patients with known CAD and LMHR should be very cautious when starting popular diets and should discuss the possible implications with their provider.
Wish they could detail what sort of ketogenic diet these patients were on.
Green heavy type?
Seed oils type?
Vegan type?
Nut heavy type?
Fruit heavy type?
Carnivore type?
Cuz the above 6 are all subsets of KD and all of them have very very different health outcomes.
So all monks and nuns got no high chlolesterol?Nature don't lies, it's humans self deceived. You have the absolute free will to choose your path and pay the price.
standarture
Great Supremacy Member
- Joined
- Feb 28, 2009
- Messages
- 61,650
- Reaction score
- 18,708
Lol veggie farming is manmade. It doesnt exist in the first place. Also eat too much got high risk of cancer. A lot of chemical pollutants.The best medicine is no need medications, just be vegetarian or vegan and it will come down naturally. Remember your alimentary canal is designed for vegetarian food..
U can eat wild grass. It is the most natural.
Dragonfly Thai black rice (aka purple rice).
https://www.fairprice.com.sg/product/dragonfly-organic-black-rice-2kg-12681560

As long as it is Thai Jasmine black rice breed, I will eat it.
Sometimes I can't find this in stock at NTUC, so the other brand is Songhe Thai black rice.
Dropping you a note to say a BIG THANK YOU for recommending me this black rice which is indeed NICE (and my two kids like it!).
First time cooking black rice (was initially worried whether it will taste 'hard hard' kind but it didnt and the texture is similar to my brown rice):
Dropping you a note to say a BIG THANK YOU for recommending me this black rice which is indeed NICE (and my two kids like it!).
First time cooking black rice (was initially worried whether it will taste 'hard hard' kind but it didnt and the texture is similar to my brown rice):
Is it soft enough? If not, try to add more water, or cook longer.
After the cook cycle is completed on the electric rice cooker, it goes into keep warm mode, and then I leave the black rice in there for at least 1 hour to keep it cooking and softening the rice.
Also the Thai jasmine black rice goes well with coconut milk.
The dessert pulut hitam mixes black glutinous rice with sugar and coconut milk.
So I found out that serving black rice occasionally with coconut milk from packet (for convenience, full version, not fat reduced), makes plain black rice even better! Try this combination. No extra sugar absolutely needed because the coconut milk itself has some sweetness in it.
lls0101
Master Member
- Joined
- Oct 24, 2015
- Messages
- 3,430
- Reaction score
- 1,797
It is always amusing seeing zealots from various food camps duking out with their own hypothesis.
Suffice to say
1) TG is an independent risk indicator for ASCVS
2) LDL is also an independent risk factor, also shown to be causative. Reduction of High LDL via lifestyle or drugs showed direct reduction in CVS mortality.
3) Apo B is a better marker of CVS risk than LDL or TG, and LDL generally correlates with Apo B, though there are cases of discordances. 90% of all Apo B is found in LDL, with the 10% in VLDL and IDL.
4) As for CVS risk of different LDL particle size, small dense LDL penetrate the endothelium more readily, but large fluffy LDL carry more atherogenic ingredient. Thus no net difference and all LDL are considered atherogenic.
5) There is no hard evidence to suggest LMHR with high LDL has a lower CVS risk than normal cohort with high LDL or high LDL is considered safe, despite all the noise in social media. It will be interesting to follow actual prevalence of CVS cases in this cohort. While waiting for this puzzle to reveal, it is important to note that there are cases of LMHR having CVS events in the literature such as below.
https://www.ahajournals.org/doi/10.1161/circ.148.suppl_1.17807
Introduction:
Ketogenic diet (KD) has been a popular diet method for weight loss and described as an alternative to pharmacotherapy on social media. KD is thought to improve some risk factors of ASCVD, such as type 2 DM, obesity, and decrease LDL. Recent studies have described lean mass hyper-responders (LMHR), a specific phenotype with lower BMI, total cholesterol >200 mg/dL, HDL >80, and TG <70. LMHR is thought to be protective against ASCVD. While on carbohydrate restricted diet, LMHR may have significant rise in LDL.
We present a patient with known CAD and similar phenotype to LMHR that developed rapid progression of CAD after stopping statin and initiating strict KD.
Hypothesis:
KD may accelerate disease in those with known CAD, despite being LMHR phenotype.
Methods:
51-year-old male with BMI 23, CAD with previous PCI to proximal LAD, HTN, HLD, family history of early CAD, presented with inferior STEMI. He underwent emergent catheterization revealing 95% stenosis of the mid RCA and 99% occlusion of the distal RCA treated with two drug eluting stents. Previous catheterization showed only moderate disease of the distal RCA. He had discontinued atorvastatin about 2 years after his first coronary intervention due to myalgias. Prior to starting it, his total cholesterol was 207, LDL 131, HDL 43, and TG 67 with a normal BMI- similar traits to LMHR phenotype. Atorvastatin 80 mg was started, and his LDL decreased to 44. After he discontinued the statin, he started a KD to try to manage his cholesterol and CAD.
Results:
When he presented with STEMI, his total cholesterol was 388, LDL 301, HDL 73, TG 71, and Lp(a) 155 nmol/L. He resumed atorvastatin 80 mg and started alirocumab at discharge with subsequent LDL of 14.
Conclusions:
Social media has influenced many to try ketogenic diet to manage metabolic health. Some influencers have questioned high-LDL association with ASCVD and have recommended avoiding pharmacotherapy. Despite popular opinion that high-LDL in this phenotype does not have clinical implication, our patient with a similar profile had rapid progression of CAD while on a KD and was untreated for HLD. Patients with known CAD and LMHR should be very cautious when starting popular diets and should discuss the possible implications with their provider.
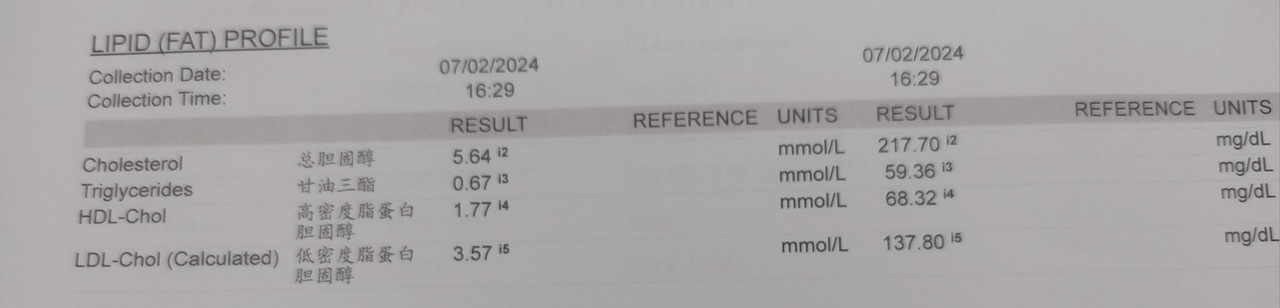
I'm also LMHR, and LDL shot up as high as 5.6 (2017) as I adopted LCHF and consume a lot more saturated fats than usual. LDL stayed high for a few years while I was on that diet.
Got my LDL lower to 2.9 (mid 2022) after I went towards plant heavy diet and greatly reduced fatty meat, sticking with leaner meat.
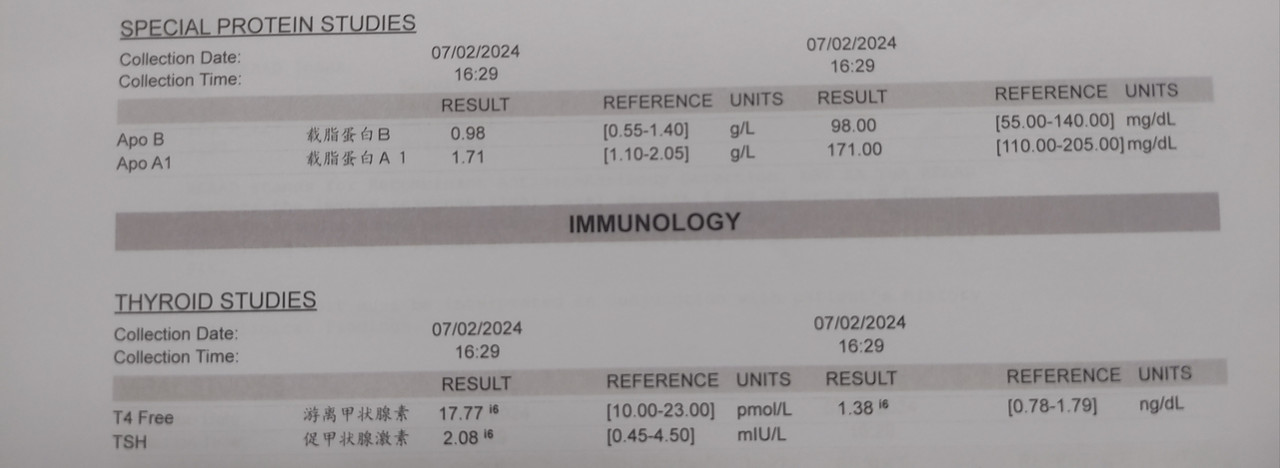
Recently did health screening and my LDL went up to borderline high as I was eating more meat for more protein and consume more fatty meat in the process. Also did ApoB and the number is within range.
How high is the risk with the increased LDL (3.5), coupled with this ApoB reading? Any advice? Thanks.

mryongtan
Arch-Supremacy Member
- Joined
- Mar 15, 2001
- Messages
- 20,920
- Reaction score
- 3,764
I also eat fish oil but still have high cholesterol despite no family history, not fat (consider slightly under weight) and I exercise everyday. I changed my diet (cut down on fried food, red meat, animal organs, food with lots of gravy) also didn't help, also prepare my own lunch on working days (mostly steam chicken and veggies) since I likely will have dinner outside.
Been taking medication (low dosage) for almost 2 years. Recently changed from simvastatin to atorvastatin since the former didn't seems to help anymore. Side effects are the same, muscle aching.
Oats actually helps but must eat constantly to have effects.
I don't believe any supplements can help.
the only way is to cut off sugars + carbs, your cholesterol would go down. you may google about it, it's a known problem.
Mecisteus
Great Supremacy Member
- Joined
- Jun 16, 2002
- Messages
- 55,069
- Reaction score
- 11,795
A research shows you need extra carbs to improve LDL assuming you are the lean mass type, physically active and have low triglycerides.the only way is to cut off sugars + carbs, your cholesterol would go down. you may google about it, it's a known problem.
https://pubmed.ncbi.nlm.nih.gov/38276308/
Generally for people who are buibui and not active with high triglycerides, then you need to cut carbs.
Mecisteus
Great Supremacy Member
- Joined
- Jun 16, 2002
- Messages
- 55,069
- Reaction score
- 11,795
I'm also LMHR, and LDL shot up as high as 5.6 (2017) as I adopted LCHF and consume a lot more saturated fats than usual. LDL stayed high for a few years while I was on that diet.
Got my LDL lower to 2.9 (mid 2022) after I went towards plant heavy diet and greatly reduced fatty meat, sticking with leaner meat.
Recently did health screening and my LDL went up to borderline high as I was eating more meat for more protein and consume more fatty meat in the process. Also did ApoB and the number is within range.
How high is the risk with the increased LDL (3.5), coupled with this ApoB reading? Any advice? Thanks.
Your numbers are similar to mine. We are physically the same.
Consider adding little carbs. Read the study I posted above.
I'm experimenting this now. Will go for a blood test next week.
My LDL can swing wildly over the years. I think because of my lean mass and carbs intake.
Mecisteus
Great Supremacy Member
- Joined
- Jun 16, 2002
- Messages
- 55,069
- Reaction score
- 11,795
I guess it's ok until they are not Ok.I saw some posts saying that having a high cholesterol is okay. Note that every single organisation on Earth says high LDL is causative of ASCVD, whether it's MOH, KKM, DOH, AHA, ACC, AAPA, ABC, ACPM, AGS, APhA, ASH, ASPC, NHC, NMA, PCNA etc
Basically if you not diabetic, physically active, low BP, low BMI but with high LDL, your risk is lower than those who are less active, high BP, diabetic and high BMI but with high LDL.
ASCVD is a multifactorial disease. You try to lower every single risk factor as much as possible.
eAtNeAt
High Supremacy Member
- Joined
- May 21, 2011
- Messages
- 40,570
- Reaction score
- 4,830
Yeah till now my parents still believe that taking white bread and rice is good and load up on them.Rmb the food pyramid? I rmb since I young HSA been pushing it. Push until diabetes everywhere in SG especially in the boomer generation.
Nowadays tell people to cut down carbs n sugars.
Let's also not forget how eggs n butter were bad, and industrial wastes like seed oils were good, and now eggs n butter are good again. Doctors even endorsed cigarettes many decades ago.
Huge beauracratic organizations takes a long time to turn around. Not the fault of individuals but that's the nature of the beast.
We as individuals can either defer our personal responsibilities(reading individual studies) by letting beauracrats do it on behalf of us, or we can seek out the information ourselves and decide.
Garmen need to be upfront and admit mistake.
lls0101
Master Member
- Joined
- Oct 24, 2015
- Messages
- 3,430
- Reaction score
- 1,797
Your numbers are similar to mine. We are physically the same.
Consider adding little carbs. Read the study I posted above.
I'm experimenting this now. Will go for a blood test next week.
My LDL can swing wildly over the years. I think because of my lean mass and carbs intake.
I'm no longer on low carb. Stopped it 4-5 years ago and my LDL drop from 5+ to 4+.
Just to make things clearer, I don't think it's the additional of carb that result in the drop of LDL from 5 to 4. It's the reduction of fatty meat for my case, I believed.
It dropped further down from 4+ to 3 when I started to go on a plant heavy diet with some very lean meat. It went up recently from 2.9 to 3.5 when I start eating more meat again (which inevitably add more fatty meat into the diet).
I think I had enough carb. Just need to reduce more meat (fatty meat), to get the LDL to 3 or below which I feel more comfortable. At least that's what works for my body as the previous results shown.
My LDL swings wildly too, greatly depending on my food consumption, based on what I observed. At least as shown in my case with the yearly results, dated from 2015 onwards...
Mecisteus
Great Supremacy Member
- Joined
- Jun 16, 2002
- Messages
- 55,069
- Reaction score
- 11,795
Saturated fats and fiber intake are part of the variables affecting LDL.I'm no longer on low carb. Stopped it 4-5 years ago and my LDL drop from 5+ to 4+.
Just to make things clearer, I don't think it's the additional of carb that result in the drop of LDL from 5 to 4. It's the reduction of fatty meat for my case, I believed.
It dropped further down from 4+ to 3 when I started to go on a plant heavy diet with some very lean meat. It went up recently from 2.9 to 3.5 when I start eating more meat again (which inevitably add more fatty meat into the diet).
I think I had enough carb. Just need to reduce more meat (fatty meat), to get the LDL to 3 or below which I feel more comfortable. At least that's what works for my body as the previous results shown.
My LDL swings wildly too, greatly depending on my food consumption, based on what I observed. At least as shown in my case with the yearly results, dated from 2015 onwards...
I'm just adding that carbs intake or balance could be another contributer if you are lean.
https://pubmed.ncbi.nlm.nih.gov/38237807/
Last edited:
Mecisteus
Great Supremacy Member
- Joined
- Jun 16, 2002
- Messages
- 55,069
- Reaction score
- 11,795
Yup this is what I have been saying.i am on inclisiran. genetic, did gene test to determine FH. no amount of dieting and exercise will help.
If you have the FH, you need the meds eventually.
Important Forum Advisory Note
This forum is moderated by volunteer moderators who will react only to members' feedback on posts. Moderators are not employees or representatives of HWZ Forums. Forum members and moderators are responsible for their own posts.
Please refer to our Community Guidelines and Standards and Terms and Conditions for more information.